When a person is working with a provider using amino acid therapy, periodic testing provides vital information to optimize neurotransmitter function as quickly as possible. Unfortunately, many providers misuse or misinterpret neurotransmitter assays, which can cause a great deal of confusion.
The Value of Neurotransmitter Testing
When properly used, testing serotonin and dopamine in the urine can dramatically improve patient outcomes. The key words in that sentence are “when properly used”, as I’ve seen many, many providers misuse and misinterpret test data, which get’s their patients no closer to optimization, nor does it speed the process towards the elimination of symptoms of neurotransmitter imbalance due to nutritional deficiency.
I’ve outlined many of the pitfalls of neurotransmitter testing elsewhere, so I won’t spend time on that here. The reason we use testing – which is really called an Organic Cation Transporter Type II Assay – is to help us determine how to adjust a person’s amino acid dosing to get them closer to optimization.
Marty Hinz, MD, is a pioneer in this field and due to his work and data-basing efforts, it’s been shown that a person’s response to amino acid therapy follows a three phase model when that person exhibits symptoms related to a serotonin relative nutritional deficiency, as shown here
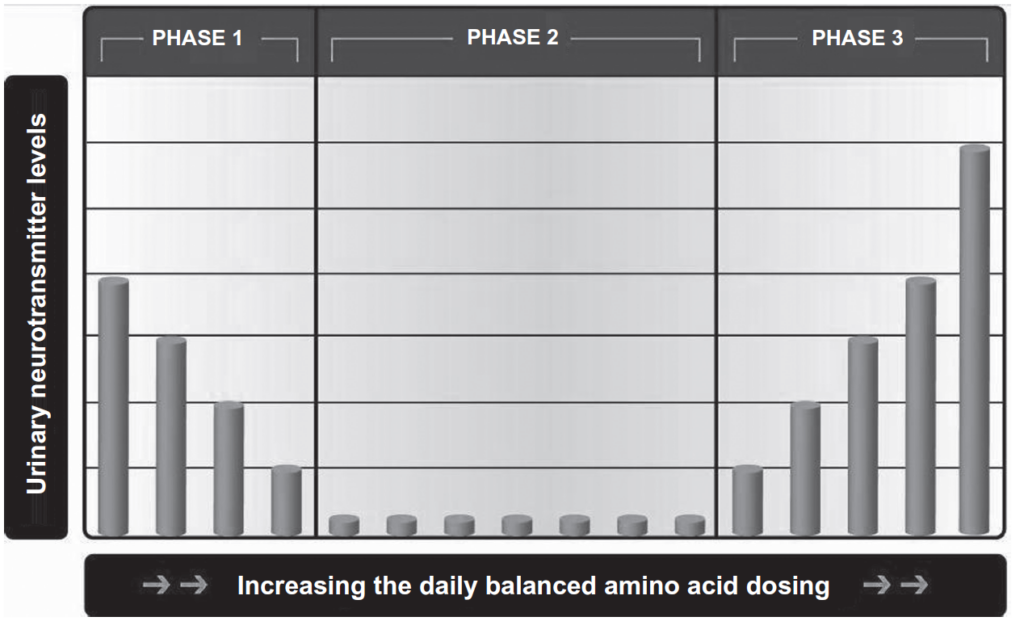
Illustration from Hinz M, Stein A, Uncini T. The dual-gate lumen model of renal monoamine transport. Neuropsychiatric Disease and Treatment. 2 July 2010.
A therapeutic response has been shown to occur when urinary serotonin and dopamine levels fall within a specific zone in Phase 3. Therefore, the information gathered during testing can be used to determine how to modify a person’s amino acid dosing to get urinary serotonin and dopamine levels closer to that zone. Typically, 2-4 tests are required for this optimization to occur.
Testing can also help the clinician to identify the small percentage of people that present with serotonin disease-like relative nutritional deficiency symptoms, but that actually require significant dopamine support (i.e., people that are dopamine dominant). In fact, without testing, properly identifying these people would not be possible.
One of the most common mistakes that I see when consulting with providers utilizing amino acid therapy is the idea that the patient cannot afford testing. The alternative that is usually chosen is to leave the patient on an amino acid dose that does not provide a relief of symptoms.
The reality is that after just one month, the cost of the supplements (which aren’t helping) outpaces the cost of testing (which can get them closer to symptom relief), so it does not make sense to postpone testing based on financial concerns. In fact, testing is necessary to achieve results as quickly as possible utilizing the exact blend of amino acids that is necessary for each person, which can actually lower supplement costs.
All this leads to a logical conclusion: work with a provider that has experience working with amino acid therapy who utilizes testing to get you the results you are looking for as quickly as possible.